
Transcription
DEPARTMENT OF CORRECTIONS
Division of Adult Institutions
DOC-1290 (Rev. 10/2011)
WISCONSIN
Wisconsin Statute
301.328 (1m)
LOAN APPLICATION
&
REPAYMENT AGREEMENT
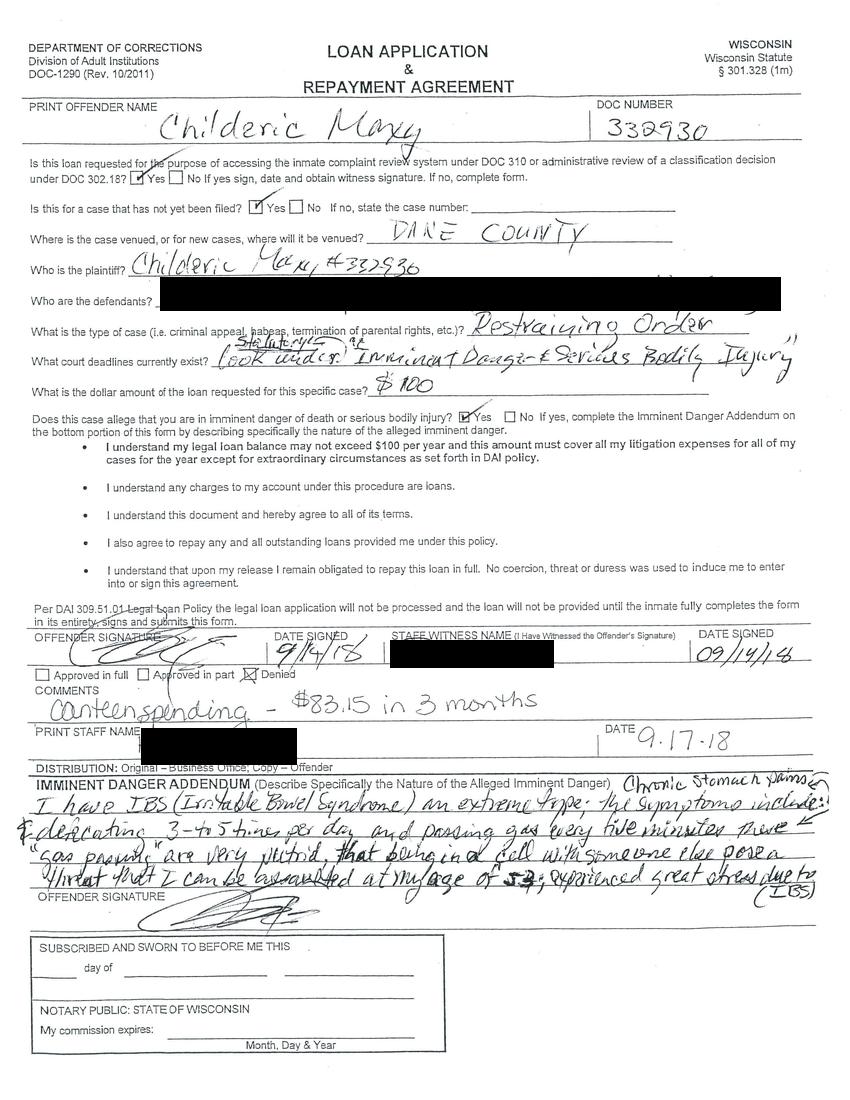
PRINT OFFENDER NAME
Childeric Maxy
DOC NUMBER
332930
Is this loan requested for the purpose of accessing the inmate complaint review system under DOC 310 or administrative review of a classification decision under DOC 302.18? [X] Yes [ ] No If yes sign, date and obtain witness signature. If no, complete form.
Is this for a case that has not yet been filed? [X] Yes [ ] No If no, state the case number:
Where is the case venued, or for new cases , where will it be venued? DARE COUNTY
Who is the plaintiff? Childeric Maxy #337930
Who are the defendants? [blanked out]
What is the type of case (i.e. criminal appeal, habeas, termination of parental rights, etc.)? Restraining order
What court deadlines currently exists? look under statutory. "Imminent danger & serious bodily injury"
What is the dollar amount of the loan requested for this specific case? $100
Does this case allege that you are in imminent danger of death or serious bodily injury? [X] Yes [ ] No If yes, complete the Imminent Danger Addendum on the bottom portion of this form by describing specifically the nature of the alleged imminent danger.
- I understand my legal loan balance may not exceed $100 per year and this amount must cover all my litigation expenses for all of my cases for the year except for extraordinary circumstances as set forth in DAI policy.
- I understand any charges to my account under this procedure are loans.
- I understand this document and hereby agree to all of its terms.
- I also agree to repay any and all outstanding loans provided me under this policy.
- I understand that upon my release I remain obligated to repay this loan in full. No coercion, threat or duress was used to induce me to enter into or sign this agreement.
Per DAI 309.51.01 Legal Loan Policy the legal loan application will not be processed and the loan will not be provided until the inmate fully completes the form in its entirety, signs and submits this form.
OFFENDER SIGNATURE
[signature]
DATE SIGNED
9/14/18
STAFF WITNESS NAME (I Have Witnessed the Offender's Signature)
[blanked out]
DATE SIGNED
09/14/18
[ ] Approved in full
[ ] Approved in part
[X] Denied
COMMENTS
Canteen spending - $83.15 in 3 months
PRINT STAFF NAME
[blanked out]
DATE
9.17.18
DISTRIBUTION: Original - Business Office; Copy - Offender
IMMINENT DANGER ADDENDUM (Describe Specifically the Nature of the Alleged Imminent Danger)
I have IBS (Irritable Bowel Syndrome) an extreme type; the symptoms include: chronic stomach pains and defecating 3 to 5 times per day and passing gas every five minutes these "gas passing" are very putrid, that being in a cell with someone else poses threat that I can be assaulted at my age of 5; experienced great stress due to (IBS)
OFFENDER SIGNATURE
[signature]
SUBSCRIBED AND SWORN TO BEFORE ME THIS
____ day of ______________ _________________
NOTARY PUBLIC: STATE OF WISCONSIN
My commission expires: ______________ Month, Day & Year
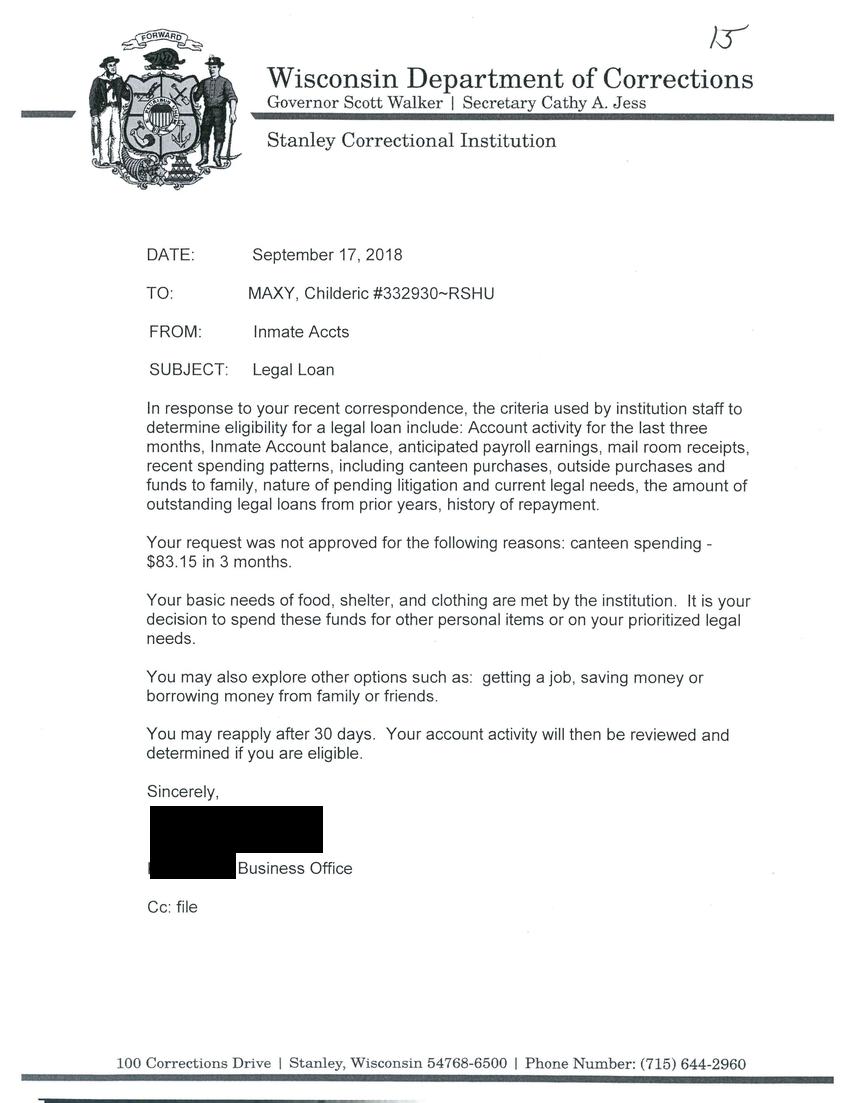
Wisconsin Department of Corrections
Governor Scott Walker | Secretary Cathy A. Jess
Stanley Correctional Institute
DATE: September 17, 2018
TO: MAXY, Childeric #332930-RSHU
FROM: Inmate Accts
SUBJECT: Legal Loan
In response to your recent correspondence, the criteria used by institution staff to determine eligibility for a legal loan include: Account activity for the last three months, Inmate Account balance, anticipated payroll earnings, mail room receipts, recent spending patterns, including canteen purchases, outside purchases and funds to family, nature of pending litigation and current legal needs, the amount of outstanding legal loans from prior years, history of repayment.
Your request was not approved for the following reasons: canteen spending - $83.15 in 3 months.
Your basic needs of food, shelter, and clothing are met by the institution. It is your decision to spend these funds for other personal items or on your prioritized legal needs.
You may also explore other options such as: getting a job, saving money or borrowing money from family or friends.
You may reapply after 30 days. Your account activity will then be reviewed and determined if you are eligible.
Sincerely.
[blanked out]
Business Office
Cc: file
100 Corrections Drive | Stanley, Wisconsin 54768-6500 | Phone Number: (715) 644-2960
DEPARTMENT OF CORRECTIONS
Division of Adult Institutions
DOC-3035 (Rev. 9/2016)
WISCONSIN
Adm. Code
Ch. DOC 316
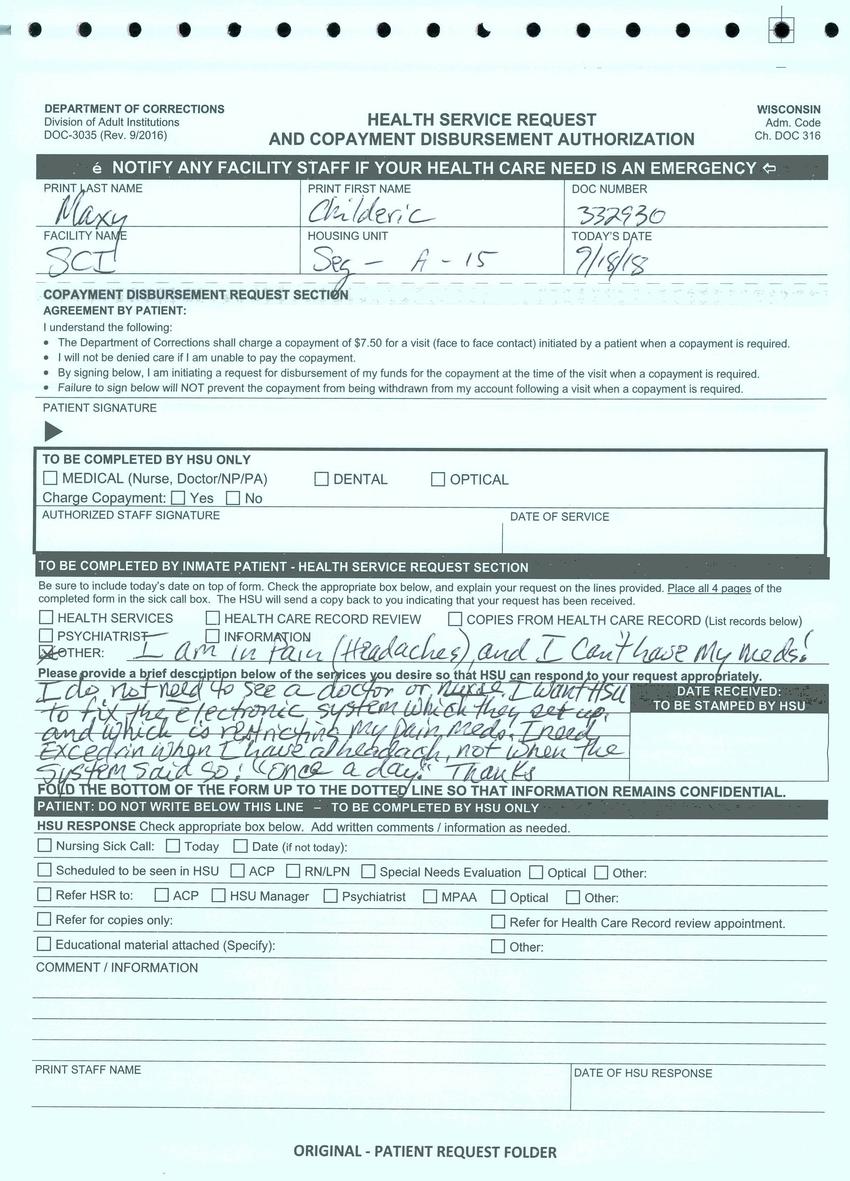
HEALTH SERVICE REQUEST
AND COPAYMENT DISBURSEMENT AUTHORIZATION
NOTIFY ANY FACILITY STAFF IF YOUR HEALTH CARE NEED IS AN EMERGENVY
PRINT LAST NAME
Maxy
PRINT FIRST NAME
Childeric
DOC NUMBER
332930
FACILITY NAME
SCI
HOUSING UNIT
Seg - A - 15
TODAY'S DATE
9/18/18
COPAYMENT DISBURSEMENT REQUEST SECTION
AGREEMENT BY PATIENT:
I understand the following:
- The Department of Corrections shall charge a copayment of $7.50 for a visit (face to face contact) initiated by a patient when a copayment is required.
- I will not be denied care if I am unable to pay the copayment.
- By signing below, I am initiating a request for disbursement of my funds for the copayment at the time of the visit when a copayment is required.
- Failure to sign below will NOT prevent the compayment from being withdrawn from my account following a visit when a copayment is required.
PATIENT SIGNATURE
TO BE COMPLETED BY HSU ONLY
[ ] MEDICAL (Nurse, Doctor/NP/PA)
[ ] DENTAL
[ ] OPTICAL
Charge Copayment: [ ] Yes [ ] No
AUTHORIZED STAFF SIGNATURE
DATE OF SERVICE
TO BE COMPLETED BY INMATE PATIENT - HEALTH SERVICE REQUEST SECTION
Be sure to include today's date on top of form. Check the appropriate box below, and explain your request on the lines provided. Place all 4 pages of the completed form in the sick call box. The HSU will send a copy back to you indicating that your request has been received.
[ ] HEALTH SERVICES
[ ] HEALTH CARE RECORD REVIEW
[ ] COPIES FROM HEALTH CARE RECORD (List records below)
[ ] PSYCHIATRIST
[ ] INFORMATION
[X] OTHER: I am in pain (Headaches) and I can't have my meds!
Please provide a brief description below of the services you desire so that HSU can respond to your request appropriately.
I do not need to see a doctor or nurse. I want HSU to fix the electronic system which they set up and which is restricting my pain meds! I need Excedrin when I have a headache, not when the system said so! "Once a day." Thanks
DATE RECEIVED:
TO BE STAMPED BY HSU
FOLD THE BOTTOM OF THE FORM UP TO THE DOTTED LINE SO THAT INFORMATION REMAINS CONFIDENTIAL.
PATIENT: DO NOT WRITE BELOW THIS LINE - TO BE COMPLETED BY HSU ONLY
HSU RESPONSE Check appropriate box below. Add written comments / information as needed.
[ ] Nursing Sick Call: [ ] Today [ ] Date (if not today):
[ ] Scheduled to be seen in HSU [ ] ACP [ ] RN/LPN [ ] Special Needs Evaluation [ ] Optical [ ] Other:
[ ] Refer HSR to: [ ] ACP [ ] HSU Manager [ ] Psychiatrist [ ] MPAA [ ] Optical [ ] Other:
[ ] Refer for copies only:
[ ] Refer for Health Care Record review appointment.
[ ] Educational material attached (Specify):
[ ] Other:
COMMENT / INFORMATION
PRINT STAFF NAME
DATE OF HSU RESPONSE
ORIGINAL - PATIENT REQUEST FOLDER
Other posts by this author
|
2026 jun 7

|
2026 jun 7

|
2026 jun 7

|
2024 aug 22

|
2024 jun 14

|
2024 feb 7

|
More... |
Replies