

Transcription
Department of Corrections
WASHINGTON STATE
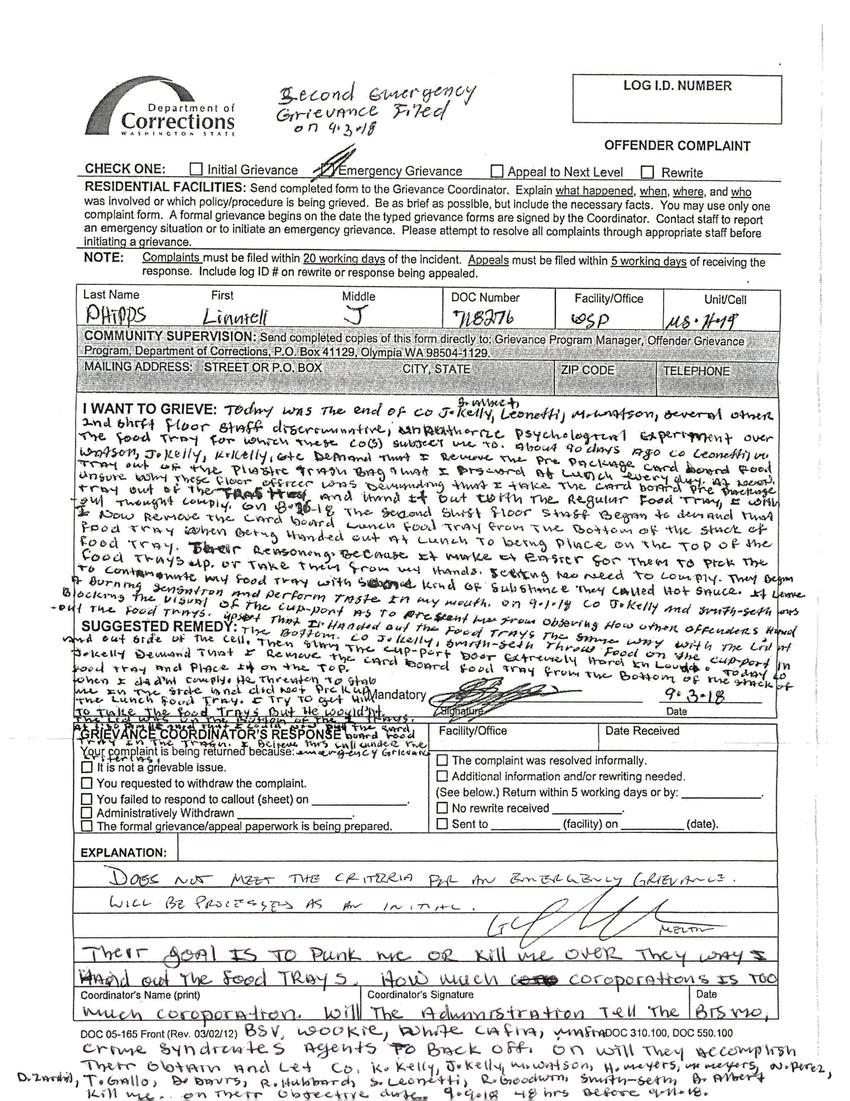
Second Emergency Grievance Filed on 9.3.18
LOG I.D. NUMBER
OFFENDER COMPLAINT
CHECK ONE: [ ] Initial Grievance [X] Emergency Grievance [ ] Appeal to Next Level [ ] Rewrite
RESIDENTIAL FACILITIES: Send completed form to the Grievance Coordinator. Explain what happened, when, where, and who was involved or which policy/procedure is being grieved. Be as brief as possible, but include the necessary facts. You may use only one complaint form. A formal grievance begins on the date the typed grievance forms are signed by the Coordinator. Contact staff to report an emergency situation or to initiate an emergency grievance. Please attempt to resolve all complaints through appropriate staff before initiating a grievance.
NOTE: Complaints must be filled within 20 working days of the incident. Appeals must be filed within 5 working days of receiving the response. Include log ID # on rewrite or response being appealed.
Last Name PHIPPS
First LINNIELL
Middle J
DOC Number 718276
Facility/Office WSP
Unit/Cell MS H79
COMMUNITY SUPERVISION: Send completed copies of this form directly to: Grievance Program Manager, Offender Grievance Program, Department of Corrections, P.O. Box 41129, Olympia WA 98504-1129.
MAILING ADDRESS: STREET OR P.O. BOX CITY, STATE ZIP CODE TELEPHONE
I WANT TO GRIEVE:
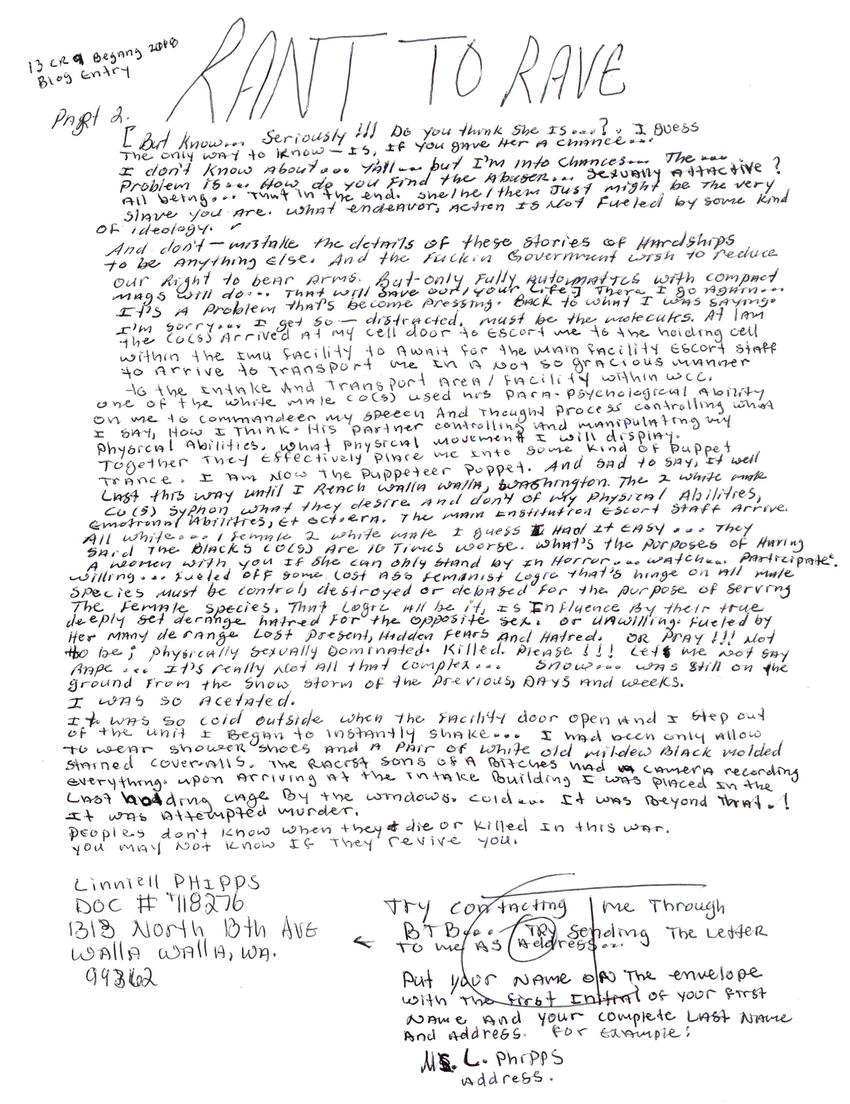
Other posts by this author
|
2019 jun 11

|
2018 dec 27

|
2018 dec 12

|
2018 dec 7

|
2018 nov 1

|
2018 sep 19

|
More... |
Replies