uploaded April 7, 2015.
Original (PDF)
Other posts by this author
|
2017 jun 24

|
2017 jun 24

|
2017 jun 24

|
2017 jun 24

|
2017 jun 18

|
2017 jun 15

|
More... |
Replies (2)
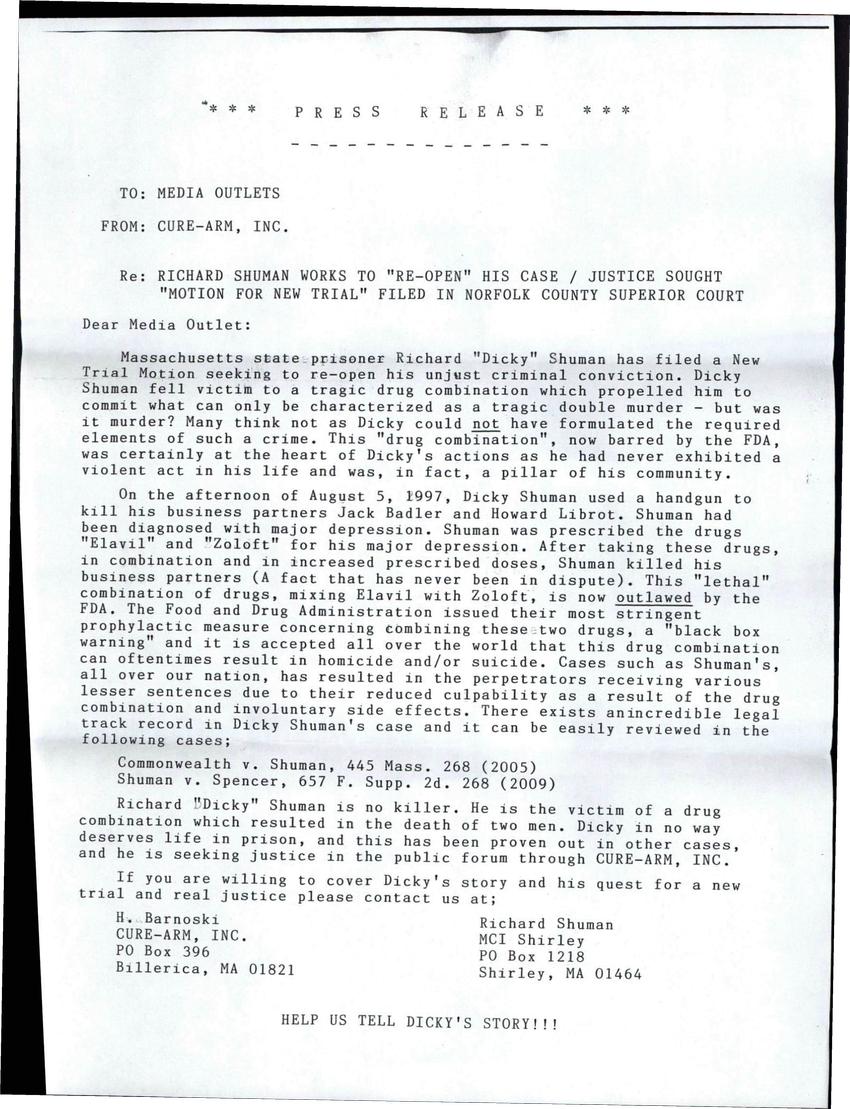
Even a simple antidepressant.
However, you say that the FDA outlaws the combination of the two drugs.
That's not true. These two drugs are still prescribed together - as far as I can see - both here and abroad (I checked in the UK, too). Doctors are told they are contraindicated (in combination) unless "the benefit outweighs the risks." So, there is a warning.
Here is what is written about using amitriptyline and sertraline (an SSRI and a tricyclic) together:
MONITOR CLOSELY: Coadministration with sertraline may increase the plasma concentrations of some tricyclic antidepressants (TCAs). The proposed mechanism is sertraline inhibition of CYP450 2D6, the isoenzyme responsible for the metabolic clearance of many antidepressant and psychotropic drugs. Moderate to significant increases (up to 250%) in plasma levels have been reported for desipramine and nortriptyline. Pharmacodynamically, the combination of sertraline (or any other selective serotonin reuptake inhibitor) and a TCA may potentiate the risk of serotonin syndrome, which is a rare but serious and potentially fatal condition thought to result from hyperstimulation of brainstem 5HT1A receptors. The syndrome has been reported in a case involving sertraline and amitriptyline.
MANAGEMENT: Caution is advised if sertraline (or other SSRIs) is prescribed with TCAs. Pharmacologic response and plasma TCA levels should be monitored more closely whenever sertraline is added to or withdrawn from therapy in patients stabilized on their existing antidepressant regimen, and the TCA dosage adjusted as necessary. Patients should be monitored closely for signs and symptoms of TCA toxicity (e.g., sedation, dry mouth, blurred vision, constipation, urinary retention) and/or excessive serotonergic activity (e.g., CNS irritability, altered consciousness, confusion, myoclonus, ataxia, abdominal cramping, hyperpyrexia, shivering, pupillary dilation, diaphoresis, hypertension, and tachycardia).
This is not to say that I understand Mr. Shuman's case or situation. But it is to say that the drug interaction CAUSING the murder is a hypothesis. I think it's something that has to be argued in court with a lot more information than just the two drugs interacting negatively.
In any case, this is slightly out of my specialty - so perhaps someone might jump in with more knowledge in this area than I have. I just wanted to track down some facts that didn't make sense to me and see what I could come up with.